
Oct. 1 marks the beginning of the fiscal year for the Centers for Medicare & Medicaid Services. This milestone does not include the changes in Medicare payments that occur with the implementation of new rules, CPT codes, or changes in the fee schedule. Those changes begin on Jan. 1 of each year, and we will once again provide you with updates in November once the final rule is published. Oct. 1 does, however, mark the new year for ICD-10.
The 2019 release includes 279 new codes, 51 deleted codes, and 143 revised codes. As of Oct. 1, 2018, there will be 71,932 active ICD-10 CM codes.
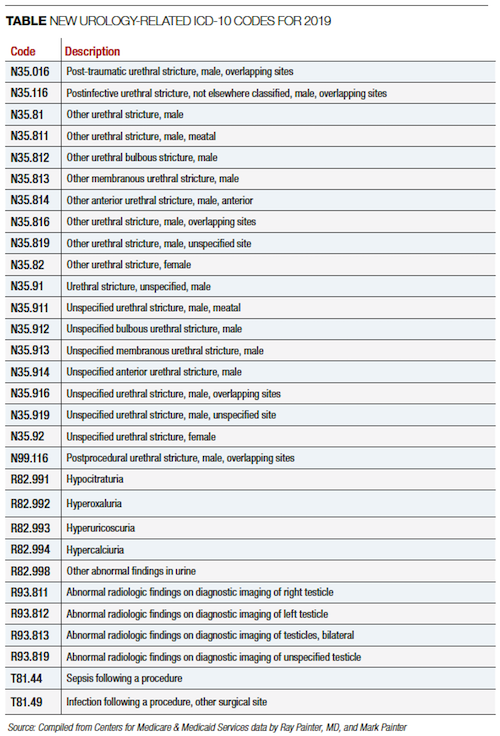

New urology-related ICD-10 codes for 2019
The table contains a list of the codes we have identified as new codes for urology. The changes are a reflection of needs identified by the World Health Organization and adapted for the U.S. under the guidance of the AUA.
Although these changes will not impact most urology practices daily, we encourage you to review them and make additions to your “favorites” lists and cheat sheets based on your practice.
Three common ICD-10 errors
While on the topic of ICD-10, we would like to highlight three common errors that we have noted in the audits we have performed throughout the year for procedural coding, office visit coding, tests, and injections. These are mistakes that are in addition to those that cause claims to be rejected due to payer rules such as local coverage determinations. Although these mistakes typically do not result in rejections of claims, they are cataloged in the payer databases and can be identified for retroactive audits and take backs.
Use of C67.9 bladder cancer site unspecified. While this code can be used if a procedure note does not specify the location from which a bladder tumor was removed, there are few cases in which the location of bladder cancer is not known with more specificity. Many urology groups we work with have noted that the site of bladder cancer typically does not change the treatment protocol with the exception of a location of the transurethral resection of bladder tumor; however, specificity is nonetheless directed by coding guidelines.
Use of symptom codes. Symptom codes are appropriate if the cause of a symptom is not yet diagnosed and the symptom is present at the time of the encounter.
Symptom codes can be used if the patient is referred for a symptom if the symptom no longer exists and if no other issue is identified for the visit. Symptom codes should be added to claims using N40.1 even if the symptom is due to BPH as instructed in the ICD-10 coding manual.
In cases where the symptom is no longer present or a diagnosis has been established and the symptom is a manifestation of the disease, it should be removed from the active diagnosis list. A great example of a misused symptom code in urology is hematuria. Any diagnosis of hematuria with a urinalysis that is clear on the same date is incorrect unless, as noted above, the patient presents with a referral for hematuria with no other symptom or disease diagnosed. A patient with hematuria due to bladder cancer with a diagnosis of bladder cancer is also incorrect.
Cancer diagnosis assigned to a patient who has undergone surgical removal of the cancer with no symptoms of the disease present. Patients who have undergone treatment for prostate, testicular, kidney, or bladder cancer for which the cancer has been removed and in whom there is no elevated PSA, remaining cancerous tissue, etc., should be diagnosed with a personal history of malignant neoplasm. this method of reporting is not only correct from a coding standpoint, but it helps you in your patient treatment statistics in the payer databases.
The other general area in which urologists need to improve their diagnosis reporting is for diseases that are chronic and/or affect the care or treatment that the patient either directly or indirectly. We have consistently taught in our seminars and articles that MIPS and the various other value-based medicine programs are looking at total cost of patient care. Your patient data risk and the statistical comparison of you and your practice to others is benchmarked to all the diagnoses a patient is assigned. Ignore these at your own peril.
We strongly recommend training your staff to assist you in coding for all relevant diagnoses for each patient, including updating any older diagnoses and adding new chronic diseases. It is often difficult to work into your daily encounters the time to add these diagnosis codes to the patient record as they typically do not have an effect on payment for that visit. But you need to understand that your long-term financial health can be adversely affected by these additional patient problems.
Add to your office work flow processes clear history forms and updates that allow you to collect this information and delegate to appropriate and well-trained staff the actions required to submit complete and accurate bills for each encounter.
ICD-10 coding is not easy if you approach each visit with a blank slate and try do all the work yourself; however, we have seen many practices develop and have assisted many others in developing processes that guide you to accurate bills with little disruption to your daily routine.
——————————————————
Photo courtesy of: Medical Coding News
Originally Published On: Urology Times
Follow Medical Coding Pro on Twitter: www.Twitter.com/CodingPro1
Like Us On Facebook: www.Facebook.com/MedicalCodingPro





